Video | Transformative Change Awards 2017: South Riverdale CHC, Sandy Hill CHC, and Parkdale Queen West CHC share honours for Supervised Injection Services

Lynne Raskin, CEO of South Riverdale Community Health Centre, speaks after accepting a Transformative Change Award for the centre's role in achieving government approval for Supervised Injection Services.
The Transformative Change Award recognizes leaders, innovators, collaborators and health champions who have been working at the forefront of transformative change helping us achieve our vision of the best possible health and wellbeing for everyone living in Ontario. On June 7, Parkdale Queen West Community Health Centre, Sandy Hill Community Health Centre, and South Riverdale Community Health Centre were recognized for their work in expanding harm reduction programs to included Supervised Injection Services.
For the past five years, Parkdale Queen West CHC, Sandy Hill CHC and South Riverdale CHC have worked to expand their longstanding harm reduction programs by adding Supervised Injection Services (SIS). Their years of hard work included collecting and presenting evidence, building partnerships, engaging communities, developing policies, preparing submissions to both the federal and provincial governments, and working with the media. Now, all three CHCs are on the cusp of getting (or have just received) government approval and funding to set up the first SIS in Ontario.
These services will undeniably save lives and help reduce risk factors that lead to infectious diseases. The fact that SIS will be located in Community Health Centres means more people who use injection drugs will have access to other much needed health and social supports. The impact of the work done by these three CHCs is already significant. Their efforts have helped shift the conversation around substance use and mental health, and enhanced the engagement in many communities towards transforming the landscape of harm reduction, drug policy and evidence-based practices.
Related Links
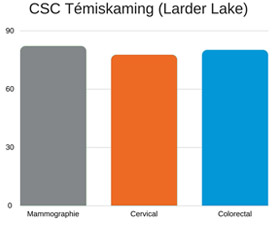 « Faire le point sur une base trimestrielle ne nous suffisait pas. Ainsi, l’attention systématique accordée au dépistage fait maintenant partie de chaque rencontre, même les renouvellements d’ordonnances », explique Roxanne Rodgers, infirmière autorisée à l’antenne de Larder Lake du Centre de santé communautaire de Témiskaming dans le Nord-Est de l’Ontario. « Notre tableau de bord de DME est simplifié de manière à regrouper tous les indicateurs au même endroit, afin que nous puissions voir rapidement quand une personne doit subir un dépistage. Ensuite, nous pouvons rédiger une requête et la lui offrir sur place. »
« Faire le point sur une base trimestrielle ne nous suffisait pas. Ainsi, l’attention systématique accordée au dépistage fait maintenant partie de chaque rencontre, même les renouvellements d’ordonnances », explique Roxanne Rodgers, infirmière autorisée à l’antenne de Larder Lake du Centre de santé communautaire de Témiskaming dans le Nord-Est de l’Ontario. « Notre tableau de bord de DME est simplifié de manière à regrouper tous les indicateurs au même endroit, afin que nous puissions voir rapidement quand une personne doit subir un dépistage. Ensuite, nous pouvons rédiger une requête et la lui offrir sur place. »