Video | Joe Leonard Award 2017: Gloria Daybutch recognized for leadership and commitment to Indigenous health

Gloria Daybutch, Executive Director of N’Mninoeyaa Aboriginal Health Access Centre, poses for a photo after receiving the 2017 Joe Leonard Award.
The Joe Leonard Award is the highest honour given by the Association of Ontario Health Centres (AOHC). Named after LAMP CHC’s first executive director, a staunch advocate for a strong, non-profit, public health care system, this award recognizes individuals who have exemplified extraordinary leadership, commitment, and support for creative solutions to accessible, quality and affordable health care. The 2017 honouree, Gloria Daybutch, embodies all those qualities and some beyond those, constantly driving herself and her staff forward to seek out new ways to deliver better programs and services to Indigenous people and communities.
Gloria has been the Executive Director of N’Mninoeyaa Aboriginal Health Access Centre since 2004. Under her leadership, the organization grew from a health department under Mamaweswen, The North Shore Tribal Council, to its current incorporated structure as Maamwesying North Shore Community Health Services Inc.
Gloria is a trailblazer when it comes to service development and design in Indigenous health. She has fostered strong working relationships with many organizations, and has worked diligently on the Aboriginal Health Care Reconciliation Action Plan. As Executive Director of Maamwesying North Shore Community Health Services, she is directly connected to the voices of the First Nation communities and the Indian Friendship Centre through the Standing Committee comprised of Health Directors.
Gloria is a Mohawk, Haudenosaune woman from the territory of Six Nations, who now resides as a member of the Mississauga First Nation. She exemplifies the values of the Seven Grandfather teachings with her humility, courage and compassion.
Related Links
Building trust and improving health services for Indigenous People


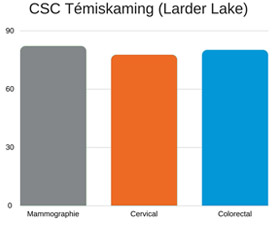 « Faire le point sur une base trimestrielle ne nous suffisait pas. Ainsi, l’attention systématique accordée au dépistage fait maintenant partie de chaque rencontre, même les renouvellements d’ordonnances », explique Roxanne Rodgers, infirmière autorisée à l’antenne de Larder Lake du Centre de santé communautaire de Témiskaming dans le Nord-Est de l’Ontario. « Notre tableau de bord de DME est simplifié de manière à regrouper tous les indicateurs au même endroit, afin que nous puissions voir rapidement quand une personne doit subir un dépistage. Ensuite, nous pouvons rédiger une requête et la lui offrir sur place. »
« Faire le point sur une base trimestrielle ne nous suffisait pas. Ainsi, l’attention systématique accordée au dépistage fait maintenant partie de chaque rencontre, même les renouvellements d’ordonnances », explique Roxanne Rodgers, infirmière autorisée à l’antenne de Larder Lake du Centre de santé communautaire de Témiskaming dans le Nord-Est de l’Ontario. « Notre tableau de bord de DME est simplifié de manière à regrouper tous les indicateurs au même endroit, afin que nous puissions voir rapidement quand une personne doit subir un dépistage. Ensuite, nous pouvons rédiger une requête et la lui offrir sur place. »